
Erectile dysfunction after robotic prostate surgery — recovery, nerve-sparing, and rehabilitation
Erections often take time to recover after radical prostatectomy — and in many men they need active rehabilitation to return. This guide explains why it happens, what nerve-sparing surgery can and cannot do, what recovery looks like, and which treatments support erectile function after surgery.
Robotic prostatectomy has changed how radical prostate surgery is performed — the precision, the magnification, the minimally invasive approach. Yet one truth remains unchanged: erections often take time to recover, and in many men they do not return to their previous level without active treatment.
That can be difficult to hear, especially when nerve-sparing surgery has been planned. The phrase sounds reassuring, and it should. Preserving the neurovascular bundles that run alongside the prostate does improve the chance of erectile recovery. But nerve-sparing is not a guarantee of normal erections after surgery — and expecting it to be often leads to unnecessary confusion and distress.
A clearer way to think about recovery is this: good surgery gives the best starting point. But recovery depends on several factors — cancer location, baseline erectile function, age, vascular health, time, and structured rehabilitation. The starting point matters. What happens next matters just as much.
Erectile dysfunction after prostatectomy is common, expected, and often temporary — but it rarely resolves without an active recovery plan. Starting rehabilitation early, with realistic expectations, gives the best results.
Why erectile dysfunction happens after robotic prostatectomy
Erections depend on finely balanced nerve signals, healthy blood flow, and responsive penile tissue working together. During a radical prostatectomy, the prostate is removed from an area where the neurovascular bundles run directly alongside the gland. Even with a robotic-assisted approach and meticulous technique, those nerves can be stretched, bruised, or temporarily disrupted during surgery.
That temporary or lasting nerve disruption reduces the signal that triggers an erection. At the same time, reduced spontaneous erections in the months after surgery may affect penile blood flow and tissue health — which is one reason structured rehabilitation starting early can make a difference to long-term outcomes.
The robotic platform supports precision, magnified vision, and careful dissection. What it cannot do is erase the fundamental anatomy or remove the need to prioritise cancer control when the tumour lies close to the nerves. Cancer clearance always takes precedence.
How nerve-sparing surgery affects erectile recovery
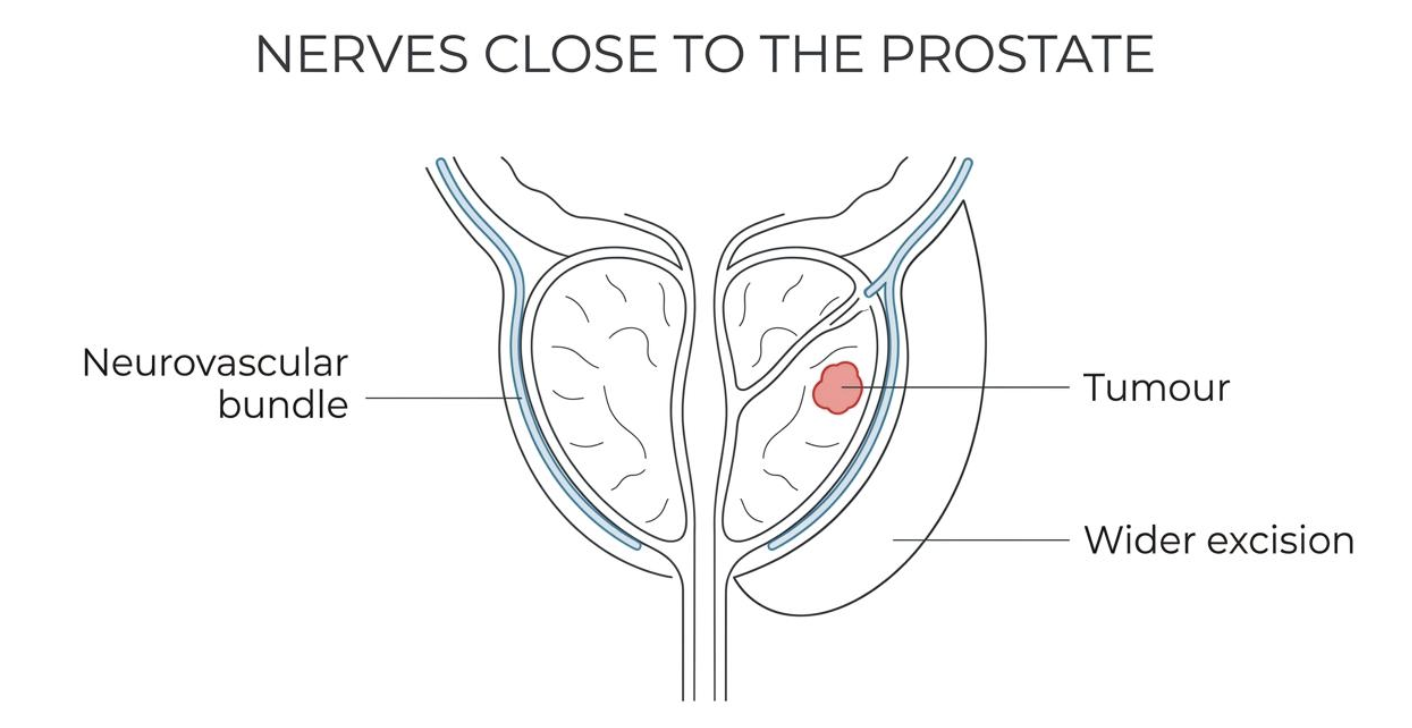
Nerve-sparing surgery aims to preserve one or both neurovascular bundles when that is oncologically safe. If the cancer appears well away from those structures, both sides may be preservable. If the cancer is close to one side, unilateral nerve-sparing may be possible. If cancer control would be compromised by preservation, wider excision is the safer choice.
Erectile outcomes are generally better after bilateral nerve-sparing than after unilateral nerve-sparing, and better after unilateral than after non-nerve-sparing surgery. Even so, recovery is highly variable. Several factors shape the likelihood of erectile recovery after robotic prostatectomy:
- Age and baseline erectile function before surgery
- Diabetes, high blood pressure, vascular disease, and smoking history
- Whether nerve-sparing is bilateral, unilateral, or not possible
- How close the cancer lies to the neurovascular bundles
- The pace and consistency of postoperative rehabilitation
A helpful framing for patients is to separate technical success from functional recovery. A surgeon may preserve the nerves carefully, yet those nerves can still take many months to recover. During that interval, erections may be absent, partial, or unreliable. That does not mean the operation has failed — it means nerve healing takes time, and the recovery process needs active support.
Typical recovery timeline
Recovery rarely follows a straight line. Some men notice little or no erectile function in the early weeks and months. Others regain partial erections first, then firmer erections later. For many, progress is slow and measured over months rather than days — and improvement beyond a year is not unusual.
This slow pace often catches patients by surprise. Urinary control typically improves earlier, while sexual function lags behind. That gap can feel discouraging, yet it reflects the biology of nerve recovery. Nerves heal slowly, and erectile function depends on more than nerve signalling alone.
| Recovery factor | What it tends to mean for erections |
|---|---|
| Strong erections before surgery | Better starting point for recovery — baseline function is the strongest predictor |
| Bilateral nerve-sparing | Higher chance of meaningful return of erectile function |
| Unilateral nerve-sparing | Recovery may still occur, though often less robust |
| Significant vascular risk factors | Slower or less complete recovery is more likely |
| Early structured rehabilitation | Supports tissue health and recovery; early start consistently outperforms waiting |
| Longer time from surgery | Improvement can continue over many months — a realistic window is 6 to 24 months |
It also matters to define what "recovery" means for you. There is a real difference between having any erection, having an erection firm enough for penetration, and feeling that sex is again spontaneous and familiar. These are not identical milestones, and honest conversation about which ones matter most should happen before surgery, not only after.
Penile rehabilitation — what it involves and when to start
Penile rehabilitation is the term used for structured treatment started after prostatectomy with the aim of supporting erectile recovery and maintaining penile tissue health. In practice, this means a structured plan rather than a single medication — and it should begin as soon as healing allows, typically within the first four to six weeks after surgery.
Common approaches include PDE5 inhibitors, vacuum erection devices, intracavernosal injection therapy, and combinations of these. NICE guidance supports access to specialist erectile dysfunction services after radical treatment for prostate cancer. That access matters because recovery after prostatectomy sits at the intersection of cancer care, sexual medicine, and emotional adjustment — and a routine follow-up focused only on PSA and continence can miss a major part of quality of life.
Mr Sri discusses erectile rehabilitation before every prostatectomy and provides a structured plan as part of post-operative care. Same-week appointments available.
Specialist follow-up and the emotional dimension
Erectile dysfunction after prostatectomy is not only a physical issue. It affects identity, relationships, confidence, and the overall sense of recovery from cancer treatment. A patient may be told the cancer is gone, yet still feel far from well because sexual function has changed so sharply.
That is why specialist follow-up matters — and why NICE recommends access to specialist erectile dysfunction services for people who have had radical treatment for prostate cancer. A specialist review can help with treatment sequencing, device teaching, prescription adjustments, injection training, psychosexual support referral, and deciding when a current plan needs changing.
The emotional dimension should not be sidelined. Performance anxiety, fear of failure, low mood, and relationship strain can amplify a physical erection problem. Counselling or psychosexual therapy can help, especially when a couple is trying to rebuild intimacy while recovery is still incomplete. Couples who communicate openly and use treatment consistently tend to cope considerably better than those who wait in silence for things to "go back to normal".
When rehabilitation is not progressing as expected, ask:
- When should tablets, devices, or injections have been started after surgery — and is it too late to begin?
- Is the current plan aimed at penile tissue health, penetrative sex, confidence, or all three — and is that the right goal for where I am now?
- At what point should lack of progress trigger a change in treatment?
- Is partner involvement, psychosexual counselling, or specialist sexual medicine referral available?
What realistic recovery looks like
The most helpful expectation is steady progress rather than instant return. Good nerve-sparing surgery improves the chance of recovery, but many men still need active rehabilitation — and some need long-term treatment. That is common, not unusual or a sign that something has gone wrong.
Progress tends to come in stages rather than all at once:
It also helps to separate sexual recovery from a narrow definition of what intimacy requires. Intimacy after prostate cancer treatment can be rebuilt while erections are still recovering. The response to erectile dysfunction after prostatectomy should not be resignation — it should be a plan that includes honest counselling before surgery, thoughtful nerve-sparing where oncologically safe, early rehabilitation, and specialist follow-up when recovery needs more support.