
The Surgeon's
Notebook
Evidence-based articles on urological conditions, robotic surgery, and what patients should know
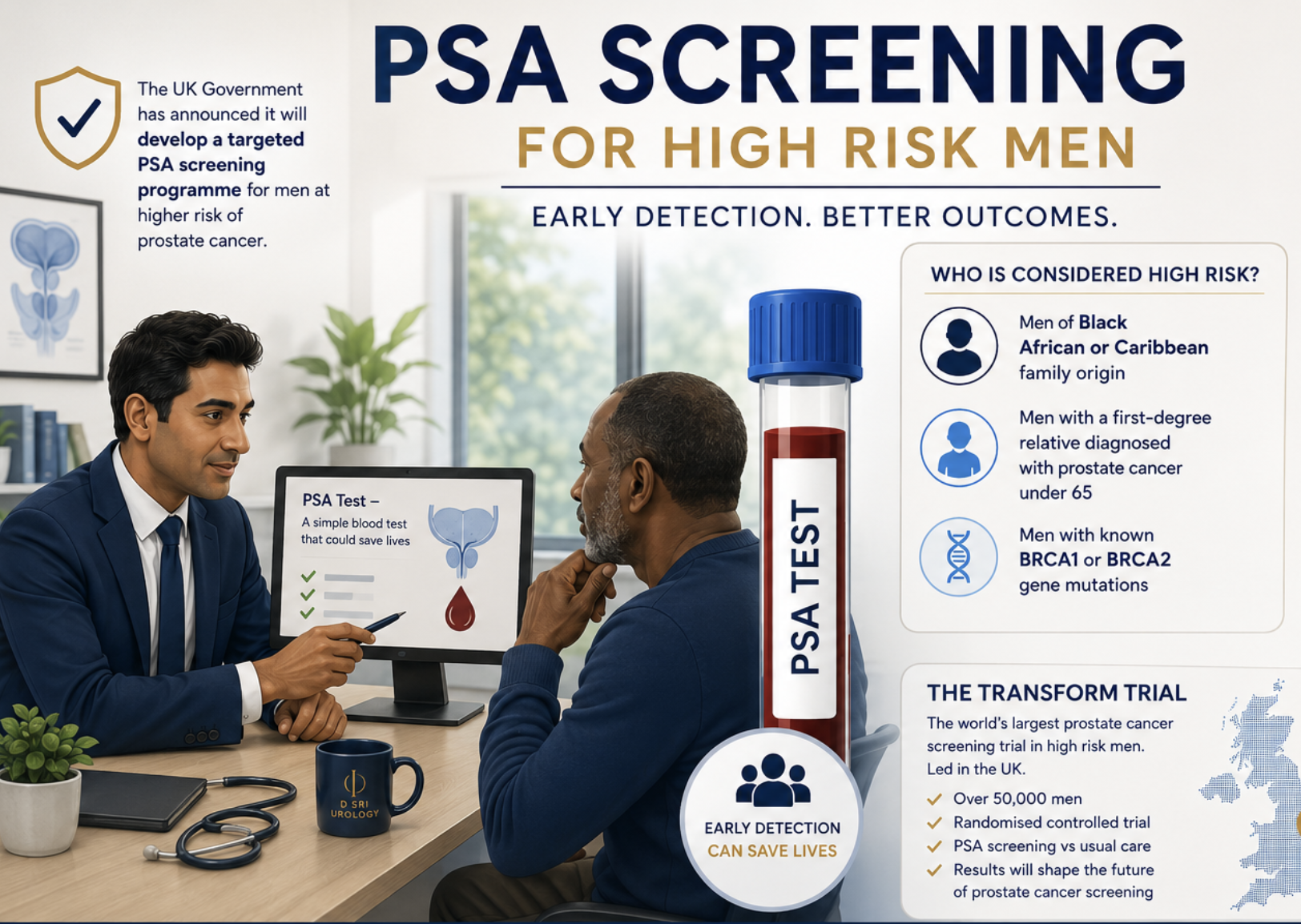
In June 2026 the government accepted England's first ever targeted prostate cancer screening recommendation — for men aged 45–61 with a BRCA2 variant and relevant family history. But most high-risk men, including all Black men without BRCA2, are still not covered. This article explains who is in the programme, who is still excluded, and what high-risk men should do right now — with an interactive tool to check your own situation.
The complete diagnostic and treatment pathway — from PSA assessment and mpMRI through to robotic prostatectomy, active surveillance, and survivorship.
Why approaching the kidney from behind — without entering the abdominal cavity — can mean faster recovery and better access to posterior tumours. Published personal outcomes included.

One in three women experience urinary incontinence. This guide covers the spectrum of treatment — from pelvic floor physiotherapy through to mesh-free robotic colposuspension — in plain language.

Blood in the urine should always prompt investigation. This guide covers what counts as haematuria, when to act urgently, and what specialist assessment involves from first appointment to diagnosis.
A raised PSA is a signal, not a diagnosis. This article explains what 5 ng/mL means at different ages, the common non-cancer causes, and the step-by-step assessment pathway.
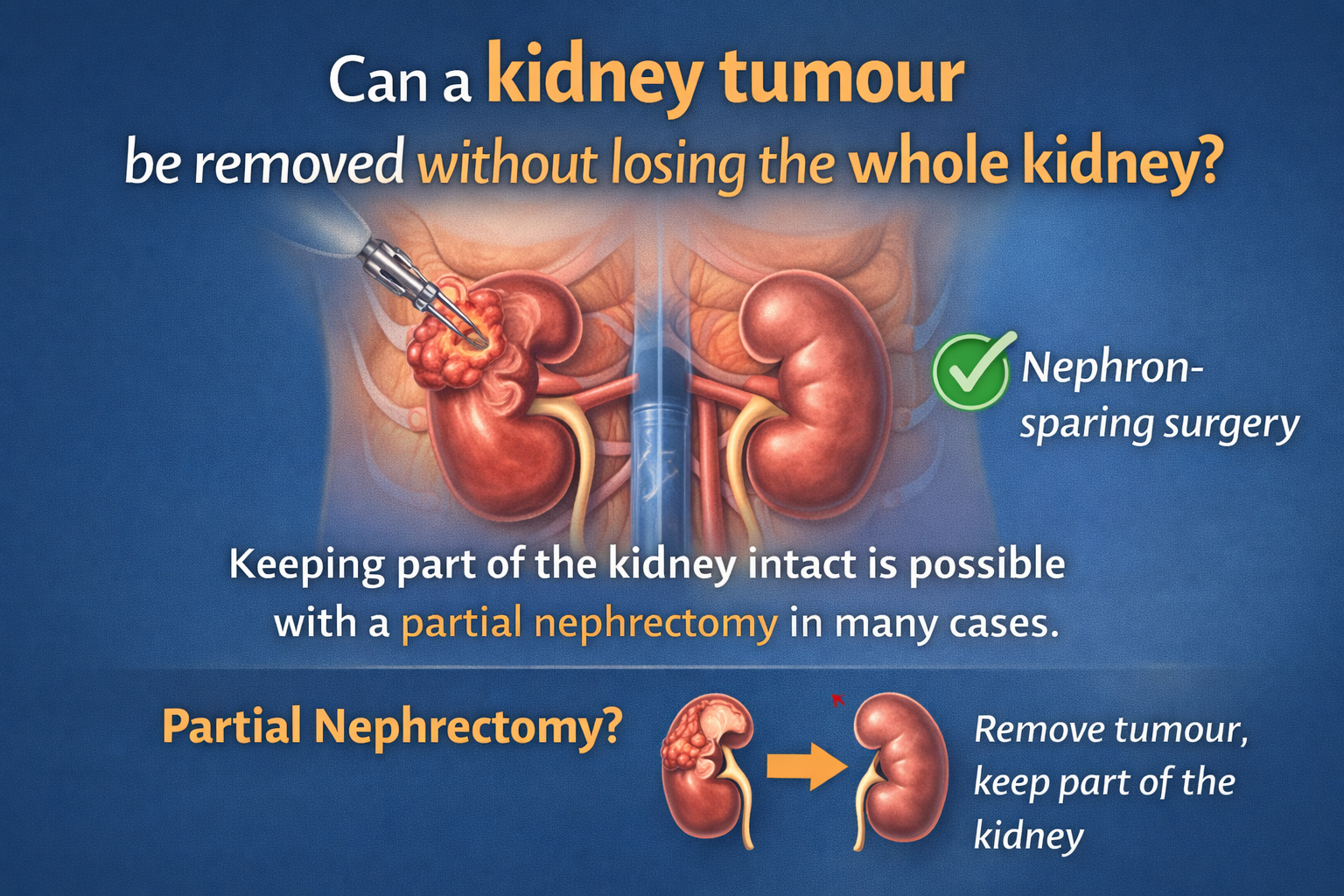
For many kidney tumours, partial nephrectomy preserves the kidney while achieving equivalent cancer control. This article explains who is suitable, how robotic surgery works, and what the decision involves.
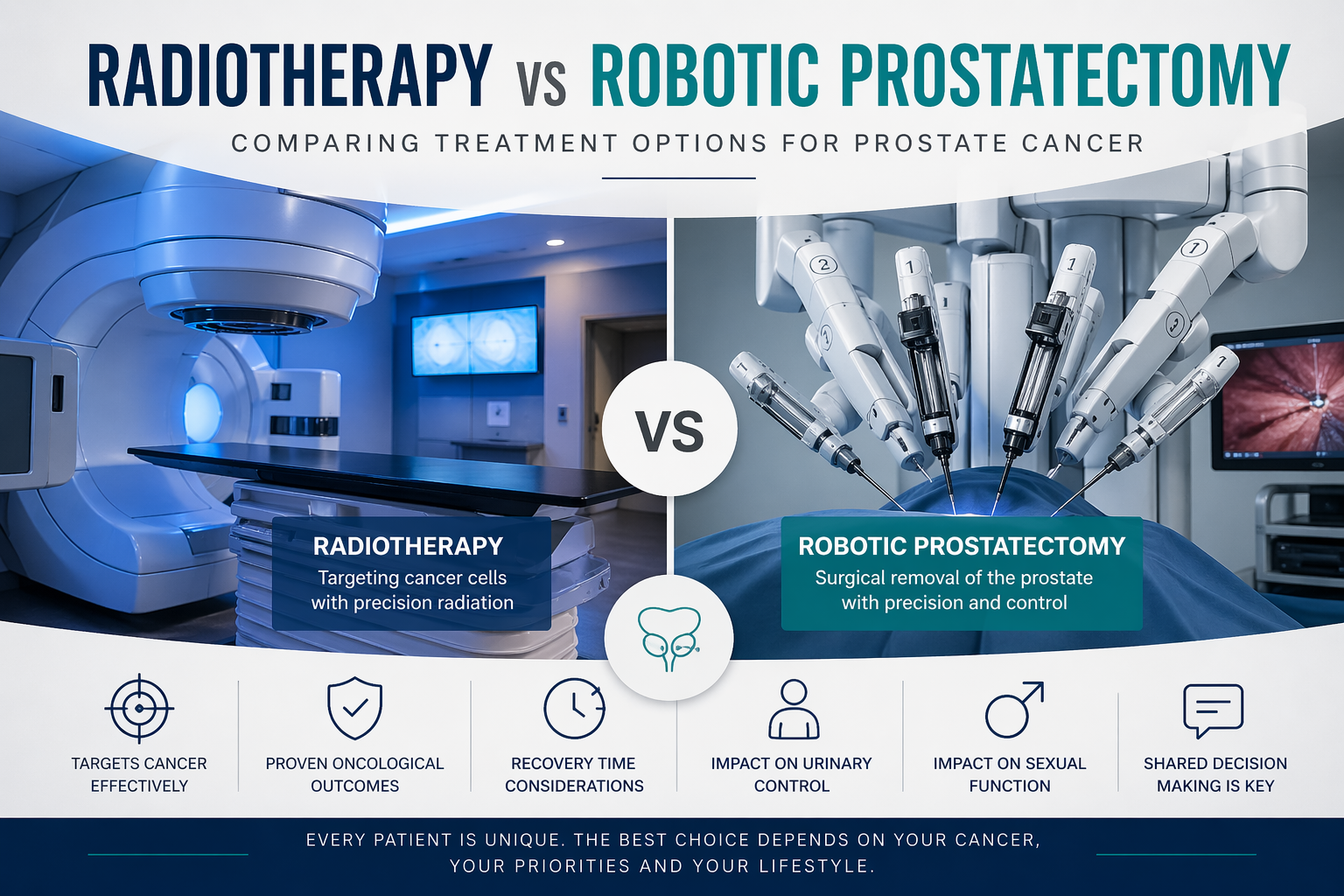
Both treatments offer equivalent cancer control for many men. The choice turns on side effects, recovery, and what trade-offs you can live with — explained clearly and honestly.
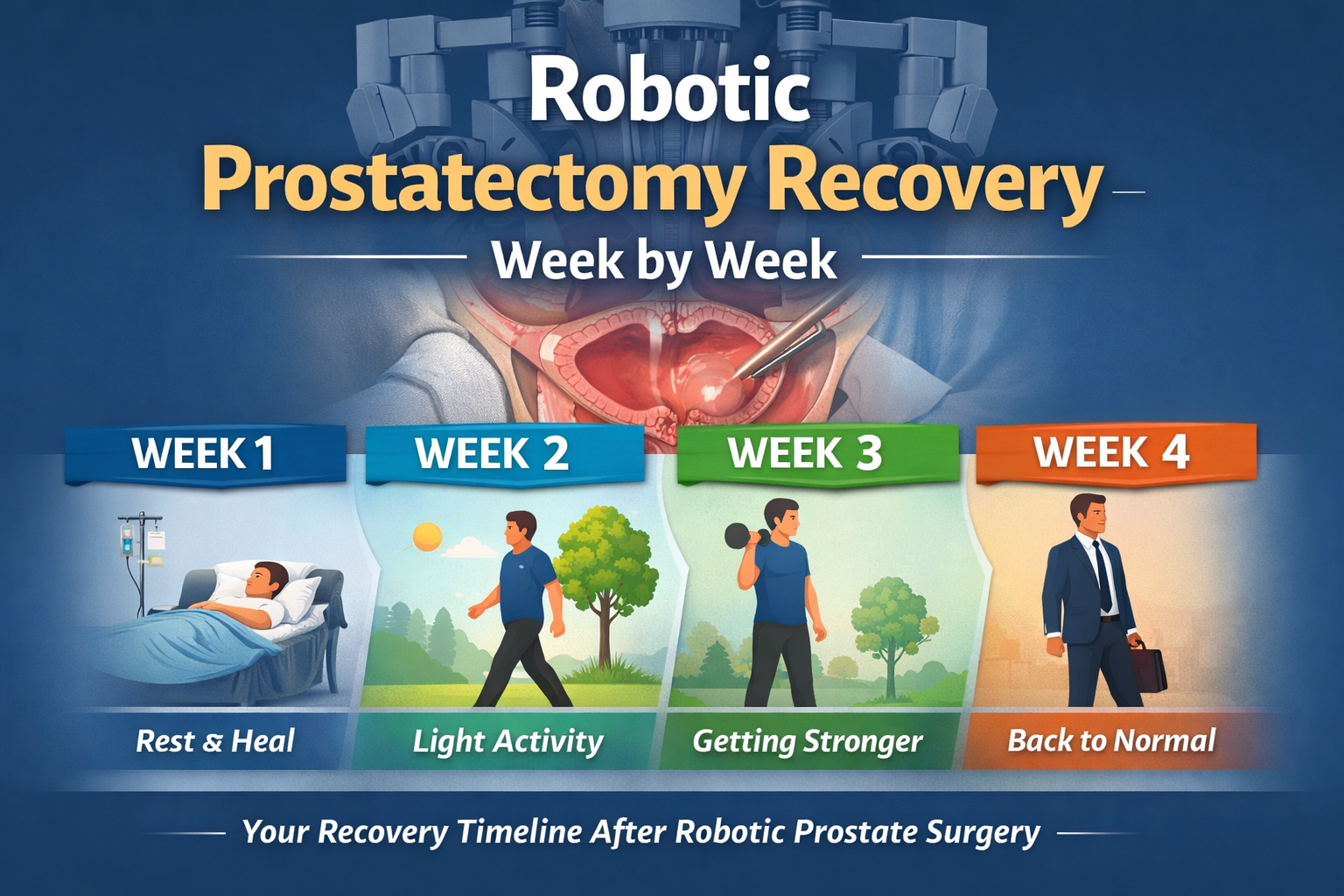
What really happens after robotic prostatectomy — catheter care, urinary leakage, PSA surveillance, penile rehabilitation, and building confidence through the first two months and beyond.
PSA 3 ng/mL sits in a genuine grey zone — below the classic referral threshold but not automatically reassuring. Age, trend, prostate size, and risk factors all determine what it means for you.
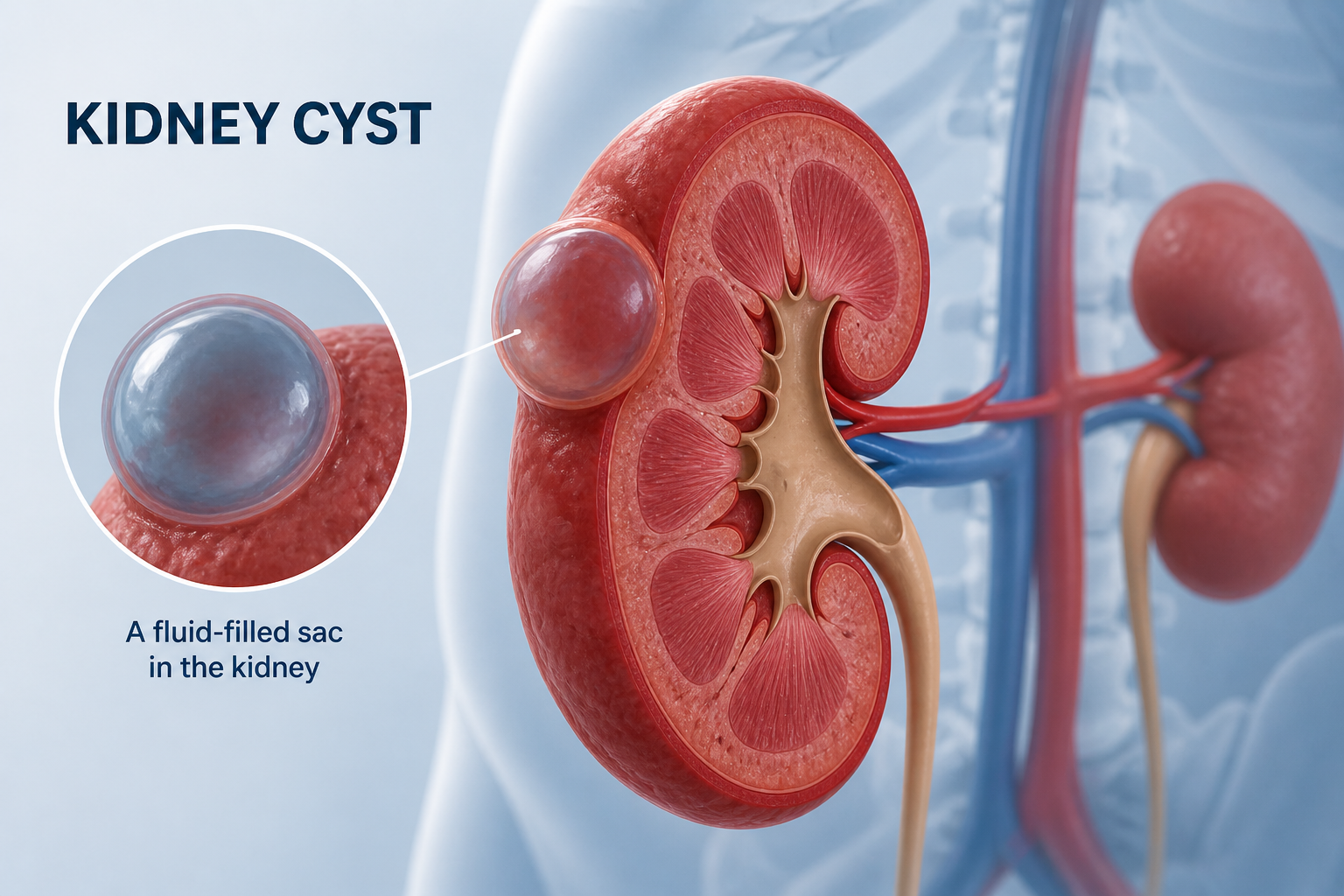
Most kidney cysts found on scans are entirely harmless. Kidney tumours are different — but many are caught early and highly treatable. This article explains what imaging shows, the Bosniak classification, and when to seek specialist review.
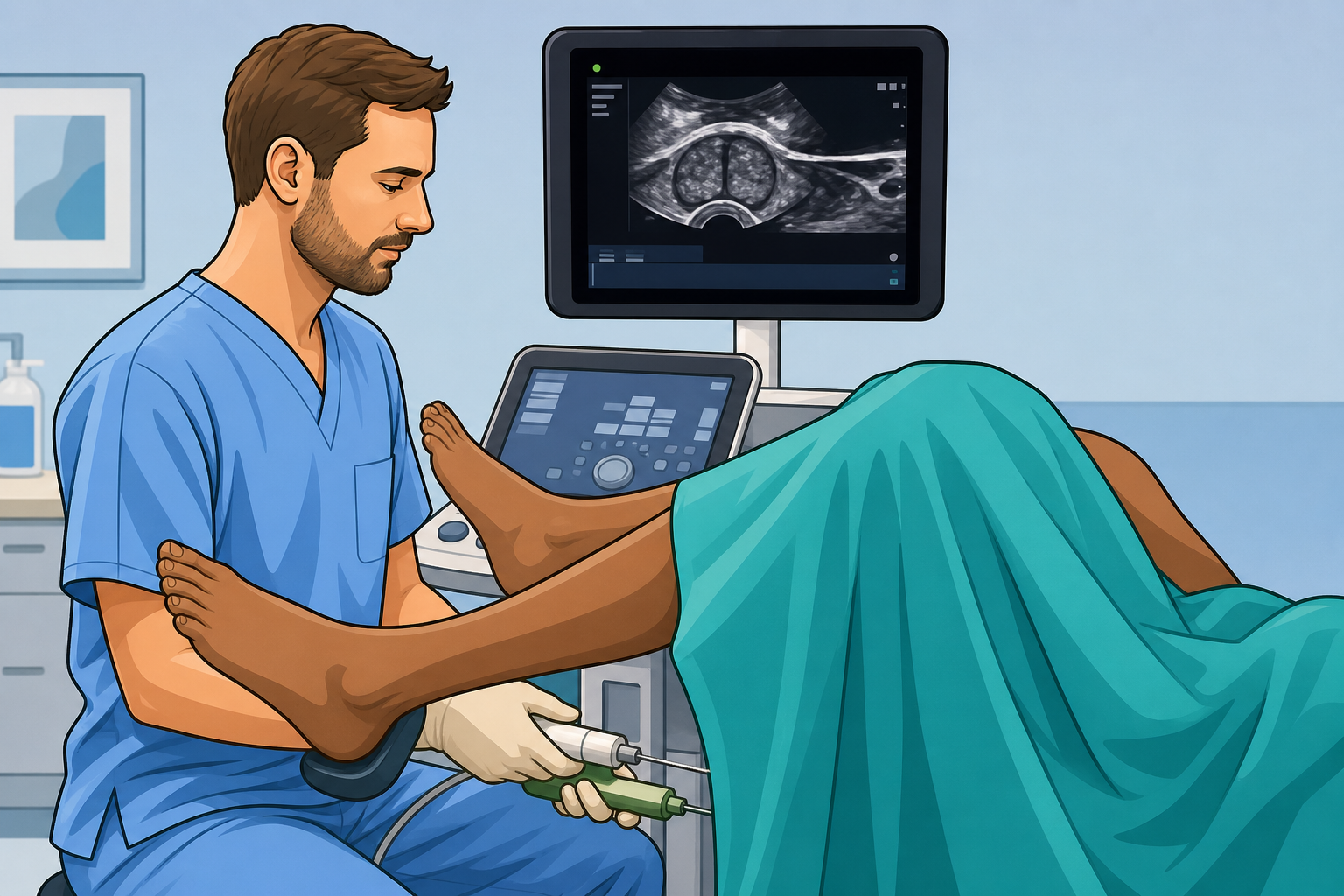
The standard approach for prostate sampling in the UK — with lower infection risk than older methods, and usually far more manageable than patients expect. A step-by-step guide to what happens and how to prepare.

All four are established BPH treatments — but they are not interchangeable. Prostate size, symptom severity, and priorities around ejaculation all determine which option fits. A plain-language guide to the differences.

A plain, honest guide to vasectomy — covering the procedure itself, what the recovery involves, when it becomes effective, and what it does not change about sexual function.
Cancer Warning signs & diagnosis
Blood in the urine is the most consistent warning sign of bladder cancer. One episode is enough to justify urgent assessment. This article explains the diagnosis pathway, cystoscopy, TURBT, and how treatment matches stage.
A PSA of 10 ng/mL is above the standard threshold and warrants prompt assessment — but it is not a diagnosis. Age, prostate size, trend, and MRI findings all shape what happens next.
Erections often take time to recover after radical prostatectomy — and many men need active rehabilitation. This guide explains nerve-sparing, recovery timelines, and the treatments that support erectile function after surgery.
The T staging letters follow a clear logic once you understand that T1 and T2 measure size, while T3 measures local spread — and a small T3 tumour (with vein involvement) can outrank a much larger T2.
The UK's first targeted prostate cancer screening programme was recommended in June 2026. It covers a tightly defined group. Most high-risk men — including Black men — are still not in a formal programme. Here is what to do.
Have a question about a urological condition?
Mr Sri sees patients at four London locations — Wimbledon, Cheam, Marylebone, and Kingston. Same-week appointments available. No GP referral required.